

Past News Items - February 2017
Return to past News items index
In the News
Study: Two-Thirds of Clinicians Lack Knowledge of Diabetes-Related Foot Complication
Can Staying Active Help to Prevent Chronic Pain? Physical Activity Affects Pain Modulation in Older Adults
78% Stroke Reduction with Newer No-Touch Beating Heart Bypass Surgery, According to Landmark Study
Study: Two-Thirds of Clinicians Lack Knowledge of Diabetes-Related Foot Complication
Diabetes can have several complications, including one common side effect: foot damage. Although some types are common, others are rarer.
Among the lesser-known conditions is Charcot neuroarthropathy.
“It is a rare foot condition that can cause significant deformity, disability and may lead to ulcerations and infections if it is not caught early in the disease process,” says Brian Schmidt, D.P.M., clinical instructor in internal medicine and member of the podiatry team at Michigan Medicine.
Commonly known as a Charcot foot and/or ankle, the effects can be debilitating.
“The joints of the foot break down, with fracture and dislocation, leading to a rocker bottom foot deformity over time,” Schmidt says. “People with peripheral neuropathy are at risk of developing this condition, and today this condition is most commonly seen in patients with diabetes mellitus. However, any patient with peripheral neuropathy is at risk.”
Many doctors, however, aren’t up to speed on the matter.
Schmidt is the lead author on a new study, published in Clinical Diabetes and Endocrinology, that investigated how much non-foot-specialist clinicians know about the condition in an effort to understand how to better focus future educational forums on the topic.
Of the 400 endocrinologists, internal medicine physicians and family medicine physicians who responded to a survey, more than two-thirds of respondents — 67.6 percent — described themselves as having poor or complete lack of knowledge of Charcot neuroarthropathy. Researchers also investigated how referring physicians treat the condition if they encounter it.
Schmidt explains what the results mean for fellow clinicians:
Why is it so important for physicians to know about Charcot neuroarthropathy, and what types of symptoms should physicians be looking for in patients?
Schmidt: Past studies have demonstrated that referring physicians can misdiagnose Charcot neuroarthropathy up to 95 percent of the time when referring the patient to a foot specialist.
This condition leads to significant morbidity and mortality and is an independent risk factor for limb loss.
Physicians should be acutely aware of the patient with peripheral neuropathy who presents to their office with sudden onset pain and a red, hot, swollen foot. This condition typically does not have any preceding event leading to a painful foot, and there may or may not be an apparent break in the patient’s skin.
What are some ways you recommend fellow physicians learn more about this complication?
Schmidt: There are many comprehensive reviews in multiple peer-reviewed journals, including a review article about the complication. Various foot and ankle societies have a plethora of information about this condition as well. Three sources of information include the American Podiatric Medical Association, Academy of Foot and Ankle Orthopedics, and the American Diabetes Association.
In addition, I am always available by email for questions or concerns.
How might patients potentially benefit from this study?
Schmidt: Patients can potentially benefit from this study by making more physicians aware of this condition. Through education about this condition, it is more likely when a patient presents to a physician with symptoms suggestive of Charcot neuroarthropathy, it will be correctly diagnosed and treated initially. If diagnosed early, many of the untoward complications can be avoided or managed effectively.
Why is it important to study this complication?
Schmidt: Although it’s a rarer complication, I see this condition on a daily basis and in various stages with significant consequences. The effects of the condition are devastating and negatively impact a patient’s life. I find that patients who have this diagnosis often don’t receive the care they need initially and this leads them down a road full of complications. Rather than treat the symptoms and sequelae of disease, I hope to improve diagnosis of this condition, leading to less complications over time.
Can Staying Active Help to Prevent Chronic Pain? Physical Activity Affects Pain Modulation in Older Adults
February 24, 2016 – Older adults with higher levels of physical activity have pain modulation patterns that might help lower their risk of developing chronic pain, reports a study in PAIN®, the official publication of the International Association for the Study of Pain (IASP). The journal is published by Wolters Kluwer.
In tests of pain processing by the central nervous system, physically active older adults have lower pain perception and are better able to block responses to painful stimuli, according to the new research by Kelly M. Naugle, PhD, and colleagues of Indiana University–Purdue University Indianapolis. "This study provides the first objective evidence suggesting that physical activity behavior is related to the functioning of the endogenous pain modulatory systems in older adults," the researchers write.
Being More Active, Less Sedentary, Affects Pain Perceptions in Older Adults
Dr. Naugle and colleagues performed a series of experiments in 51 healthy adults, aged 60 to 77. All wore an activity monitor device for one week to measure their level of physical activity. They then underwent two tests of pain modulation—functions affecting the way pain is interpreted and perceived by the central nervous system.
One test, called "temporal summation," measured the production (facilitation) of pain responses to repeated pain stimuli. The other test, called "conditioned pain modulation," assessed the reduction (inhibition) of pain responses to competing pain stimuli.
In both tests, pain modulation was significantly related to daily physical activity level. Older adults with more frequent moderate-to-vigorous physical activity had lower pain scores on the temporal summation test—indicating less pain facilitation. Those who did more light physical activity or had less sedentary time per day had lower pain scores on the conditioned pain modulation test—indicating better pain inhibition.
In other words, older adults who did more moderate to vigorous physical activity perceived less facilitation of pain, while those who did at least some activity were better able to block pain perceptions. These differences may be relevant to the "central sensitization" process believed to be responsible for the transition from acute to chronic pain.
Previous studies have shown that pain modulation processes are dysregulated in patients with chronic pain syndromes—for example, arthritis, back pain, and fibromyalgia. People with higher pain facilitation and lower pain inhibition are more likely to develop problems with chronic pain.
The results are consistent with studies in younger adults suggesting that higher levels of physical activity are related to "more efficient conditioned pain modulation." Older adults are more likely to be physically inactive, which might make them more vulnerable to chronic pain.
"Our data suggest that low levels of sedentary behavior and greater light physical activity may be critical in maintaining effective endogenous pain inhibitory function in older adults," Dr. Naugle and coauthors write. Further studies will be needed to test the implications for physical activity programs to reduce and prevent pain in older adults. For example, it might be possible to match the patient's specific dysfunctional pain modulation pattern to the type of physical activity that can best improve their pain response patterns.
Wolters Kluwer Health is a leading global provider of information and point of care solutions for the healthcare industry. For more information about our products and organization, visit www.wolterskluwer.com.
78% Stroke Reduction with Newer No-Touch Beating Heart Bypass Surgery, According to Landmark Study
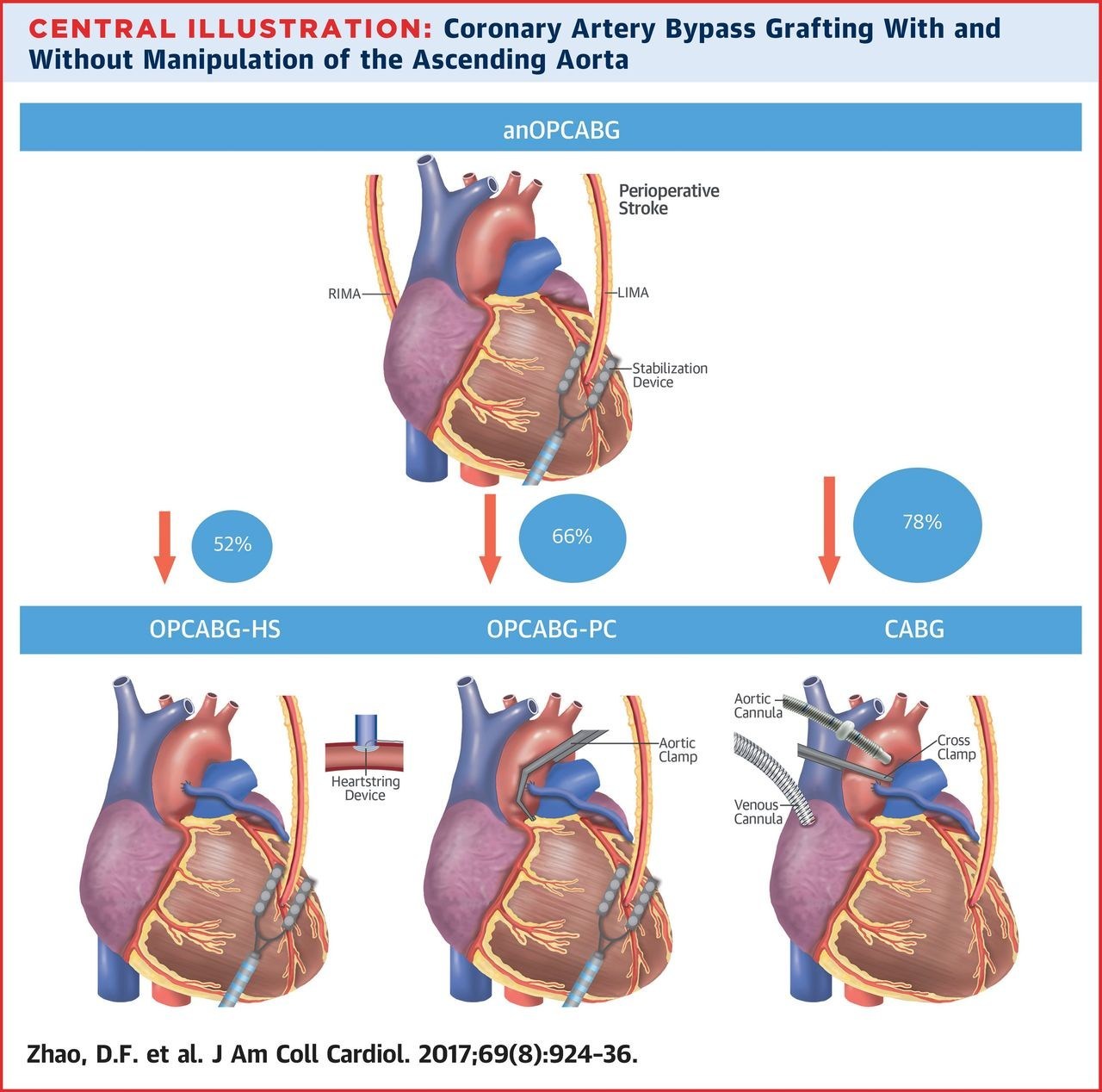
A landmark study led by Prof. Michael P. Vallely, MBBS, PhD, FRACS, of Sydney Heart and Lung Surgeons and the University of Sydney will be published in the February 28, 2017 issue of the Journal of the American College of Cardiology. According to the study, which involved 37,720 patients, a newer "no-touch" beating heart bypass surgery technique (anOPCABG) reduced postoperative stroke by 78% compared to traditional coronary artery bypass grafting (CABG). In addition, compared to traditional CABG, the newer "no-touch" technique also reduced postoperative mortality by 50%, renal failure by 53%, bleeding complications by 48%, atrial fibrillation by 34%, and length of intensive care unit stay by 13.3 hours. The co-authors of this study included world-renowned cardiothoracic surgeons from Australia, the United States, Canada, and the United Kingdom.
Coronary artery bypass grafting (CABG) is a surgical procedure for ischemic heart disease, which is the most common cause of death in Western countries. In this disease, the gradual build-up of fat and calcium within the arteries of the heart causes narrowing, which reduces blood flow to the heart's muscle. When the narrowing becomes very severe or completely blocked it causes a heart attack.
{kind=link}
Four surgical methods of coronary artery bypass grafting with increasing degrees of aortic manipulation. Percentages pictured represent the relative decrease in risk of perioperative stroke using anOPCABG compared to the other techniques. CABG = coronary artery bypass grafting with cardiopulmonary bypass; anOPCABG = anaortic off-pump coronary artery bypass grafting; LIMA = left internal mammary artery; OPCABG-HS = off-pump coronary artery bypass grafting with the Heartstring system; OPCABG-PC =...
CABG involves bypassing these blockages using a graft. The graft goes around the blocked artery to create new pathway for oxygen-rich blood to flow to the heart again. The aim of this is to relieve symptoms (including angina), help the patient resume a normal lifestyle, and to prevent the risk of heart attacks or other heart problems. However, traditional CABG involves stopping the heart during surgery and placing a clamp on the large vessel of the heart (aorta).
Sewing the grafts to the heart is traditionally performed on a still, non-beating heart while the patient is on a heart-lung machine ("on-pump surgery"). In contrast, the newer no-touch, off-pump technique is performed on a beating heart without the heart-lung machine, using a small stabilizer. Since the heart-lung machine is not needed, the large vessels of the heart do not need to be manipulated (an "anaortic" or "no-touch" technique). This technique particularly benefits elderly and high-risk patients, and was shown in this new study to reduce the risk of stroke, death, and kidney injury following the operation.
The no-touch beating heart technique performed "without aortic manipulation, whilst performed only by a minority of surgeons, has an important place in the higher risk patient undergoing CABG," commented Prof. Michael P. Vallely, corresponding author of the study and cardiothoracic surgeon at Sydney Heart and Lung Surgeons, "this powerful analysis demonstrates the potential benefit, not only in the reduction of stroke, but also in mortality... [and] provides the most comprehensive and highest-quality evidence currently available [to] help inform decisions regarding the management of these patients."
"Interestingly, the risk of stroke seemed to be directly related to the extent of aortic manipulation," said John G. Byrne, MD, of Hospital Corporation of America and Marzia Leacche, MD, of Spectrum Health in an editorial for the Journal of the American College of Cardiology, "a no-touch technique is probably a superior approach compared to conventional on-pump CABG with aortic clamping... in patients with increased cerebrovascular disease or atherosclerotic disease in the aorta."
About the Study
For the first time, an advanced Bayesian network model has been utilized to directly compare the clinical outcomes of all the major coronary artery bypass grafting techniques, including a totally anaortic or "no touch" off-pump technique, off-pump with a partial-clamp, off-pump with the clampless Heartstring device (St. Jude Medical, Saint Paul, Minnesota), and traditional on-pump with cross-clamp technique. This study will be published in the February 28, 2017 issue of the Journal of the American College of Cardiology.